
Primary Sclerosing Cholangitis
Patient.info
Primary sclerosing cholangitis is an uncommon condition affecting the bile ducts and liver. Inflammation and scarring of the bile ducts can lead to liver damage and cirrhosis – a condition where normal liver tissue is replaced by scar tissue (fibrosis). Different treatments are available to control symptoms that may develop and also to manage any complications which may occur. The outlook for people with primary sclerosing cholangitis can be very variable.
What does the liver do?
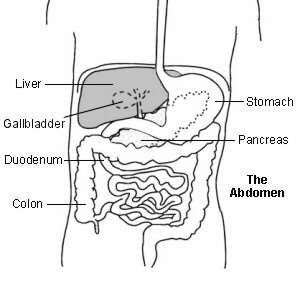
The liver is in the upper right part of the tummy (abdomen). It has many functions which include:
- Storing glycogen (fuel for the body), which is made from sugars. When required, glycogen is broken down into glucose which is released into the bloodstream.
- Helping to process fats and proteins from digested food.
- Making proteins that are essential for blood to clot (clotting factors).
- Processing many medicines which you may take.
- Helping to remove or process alcohol, poisons and toxins from the body.
- Making bile, which passes from the liver to the gut down the bile duct. Bile breaks down the fats in food so that they can be absorbed from the bowel.
What are bile and bile ducts?

Bile is a yellow-green liquid that contains various chemicals and bile salts. Bile helps you to digest food, particularly fatty foods. It also helps the body to absorb certain vitamins (A, D, E and K) from the food that you eat.
Bile is made by liver cells. Liver cells pass out bile into a network of tiny tubes called bile ducts. They join together (like tributaries of a river) to form the larger common bile duct. Bile constantly drips down the tiny bile ducts, into the common bile duct, and into the first part of the small intestine (which is called the duodenum).
The gallbladder lies under the liver. It is like a pouch off the common bile duct and fills with bile. It is like a reservoir that stores bile. The gallbladder squeezes (contracts) when we eat, as the bile is needed to aid digestion. This empties the stored bile back into the common bile duct and out into the duodenum.
What is primary sclerosing cholangitis (PSC)?
PSC is an uncommon condition that affects the bile ducts and liver. It is called:
- Primary – because the cause is not known. (That is, it is not ‘secondary’ to any known cause such as alcohol or poisons.)
- Sclerosing – because it causes scarring and thickening (sclerosis) of the bile ducts.
- Cholangitis – which means inflammation of the bile ducts.
In this condition, the bile ducts both inside and outside the liver become inflamed and scarred. The scarring causes narrowing of these bile ducts which results in bile building up in the liver. The bile can then damage the liver cells. Eventually, the scar tissue can spread throughout the liver, causing cirrhosis and liver failure. Cirrhosis is a serious condition where normal liver tissue is replaced by scar tissue (fibrosis). It tends to progress slowly and often does not cause symptoms in its early stages. However, as the function of the liver gradually becomes worse, serious problems can develop. See separate leaflet called Cirrhosis for more details.
What causes primary sclerosing cholangitis (PSC)?
The cause is not clear. It can sometimes run in families. Around four out of five people with PSC also have inflammatory bowel disease (most often ulcerative colitis, but it can also be associated with Crohn’s disease).
Note: most people with inflammatory bowel disease (ulcerative colitis or Crohn’s disease) do NOT develop PSC.
Who develops primary sclerosing cholangitis (PSC)?
PSC is rare. It can occur at any age but is more common in people aged around 40 years. It is twice as common in men as in women.
What are the symptoms of primary sclerosing cholangitis (PSC)?
In many cases the symptoms develop gradually over weeks or months. At the beginning of the disease, many people have no symptoms at all. The most common early symptoms include feeling more tired than usual, feeling generally unwell, itchy skin, weight loss and having some discomfort in the right upper tummy (abdomen).
Jaundice can develop when the condition worsens. If you have jaundice, you ‘go yellow’. You tend to notice it first when the whites of the eyes become yellow. This is due to a build-up of the chemical bilirubin, which is made in the liver and, in some liver conditions, spills into the blood.
What are the complications of primary sclerosing cholangitis (PSC)?
Various complications can occur in some people with PSC. These include:
- Deficiencies of some vitamins, usually vitamins A, D, E and K. These are the vitamins which are fat-soluble (rather than the other vitamins which are water-soluble). This means they dissolve in fat. Bile helps the fat to be broken down and these vitamins to be absorbed.
- Infection of the blocked bile ducts. This is called infective cholangitis. This may cause chills, fever and upper tummy (abdominal) tenderness.
- Cirrhosis – where normal liver tissue is replaced by scar tissue (fibrosis).
- Liver failure.
- Bile duct cancer. This eventually affects around 1 in 10 people who have PSC.
Diagnosing primary sclerosing cholangitis (PCS)
Many people with PSC have no, or only vague, symptoms for quite some time in the early stages of the disease. Therefore, the diagnosis is often made when you have tests for an unrelated condition or routine tests if you have inflammatory bowel disease.
Tests usually include:
- Blood tests called liver function tests. These measure the activity of chemicals (enzymes) and other substances made in the liver. This gives a general guide as to whether the liver is inflamed and how well it is working. See separate leaflet called Liver Function Tests for more details.
- Other blood tests may be performed to rule out (exclude) other causes of liver conditions such as viral hepatitis.
- An ultrasound scan of the liver may be performed.
- A cholangiogram is a test which produces a picture of the bile ducts. This is often done using an MRI scan.
- Taking a small sample (biopsy) of the liver. This may be carried out to look at the sample under the microscope. It can show inflammation and the extent of any cirrhosis (where normal liver tissue is replaced by scar tissue (fibrosis) in the liver). The liver biopsy can also assess how early or advanced the disease is. See separate leaflet called Liver Biopsy for more details.
What is the treatment for primary sclerosing cholangitis (PSC)?
At present there is no specific treatment which either cures or slows the progression of PSC. Treatments aim to improve symptoms and also to manage any complications which may arise.
Treatment of symptoms
Itching of the skin can be difficult to treat but is usually eased with a medicine called colestyramine. Other medicines may be tried if this is not effective.
Medical treatment
There is no effective medical treatment apart from using medicines to ease symptoms. Vitamin supplements may be advised.
Treatment of complications
Antibiotics will be given if you have an episode of infective cholangitis. If your cholangiogram shows that you have an obstruction to the bile duct outside your liver, it may be possible for a doctor to place a small drainage tube (a stent) or use a very small balloon to open up the blockage.
Liver transplant
If your liver is affected badly then you may be considered for a liver transplant. Outlook following a liver transplant is good. However, PSC recurs in around a fifth of cases following a liver transplant.
Diet and alcohol
Most people with primary sclerosing cholangitis (PSC) will be advised to eat a normal healthy diet. Ideally, anybody with inflammation of the liver should not drink alcohol, or only in very small amounts. If you already have liver inflammation, alcohol may increase the risk and speed of developing cirrhosis – where normal liver tissue is replaced by scar tissue (fibrosis).
What is the outlook (prognosis)?
The course of primary sclerosing cholangitis (PSC) is variable. There is also an increased risk of developing cancer of the bile duct (cholangiocarcinoma) or bowel (colorectal) cancer.
The treatment of PSC is a developing area of medicine. New treatments continue to be researched and the information above is very general. The specialist who knows your case can give more accurate information about the outlook for your particular situation.
___
https://patient.info/health/abnormal-liver-function-tests-leaflet/primary-sclerosing-cholangitis