
A practical guide to compatibility testing for dental materials.
Steve Koral, DMD, MIAOMT
IAOMT
 As biologically-minded dentists, we strive to achieve all the goals of modern dentistry while treading as lightly as possible on our patients’ biological terrain. So while we work to maximize strength, durability, comfort and esthetics, we seek to minimize toxicity, immune reactivity, and galvanic stress.
As biologically-minded dentists, we strive to achieve all the goals of modern dentistry while treading as lightly as possible on our patients’ biological terrain. So while we work to maximize strength, durability, comfort and esthetics, we seek to minimize toxicity, immune reactivity, and galvanic stress.
The restorative materials we use today have all been developed with “most people” in mind. Most people can put up with a bit of toxicity, immune reactivity and galvanic stress. However, there are outliers, and perhaps their numbers are growing, who can’t stand up to those stresses as well as others. The prevalence of multiple chemical sensitivities (MCS) has been reported to be somewhere between 12 and 33% in the general population, with 2 to 6% having been actually diagnosed as such.
There is a well documented physiological basis for MCS. Genetic variations leave some people with low-functioning enzymes in critical detoxification pathways, such as methylation, phase-2 conjugation, reduction of oxidized glutathione, membrane transport, and others. The result is that they can’t excrete the chemicals they are exposed to effectively, and essentially are poisoned. Some researchers have suggested that there are psychological components to the disease as well. Certainly the experience of MCS leads to fear of exposure in the hearts of these patients, including fear of dental materials.
Moreover, there is a significant number of people who are overtly allergic, or otherwise immunologically reactive, to chemicals in their environment. This phenomenon ranges from true allergies to something akin to non-allergic food sensitivities. It results in a range of idiosyncratic, highly individual immune reactions in susceptible people.
These people tend to know who they are, and they are immensely grateful when their dentist acknowledges the problem when prescribing dental materials. After all, people can manage food sensitivities by rotating the diet, but they can’t rotate their permanently installed artificial dental fillings. By practicing individualized biocompatibility testing, and making other common sense choices, we can (almost) always find a combination of professionally recognized restorative materials that will do the job. We can fix teeth and at the same time help our patients avoid toxicity, immune reactivity, and galvanic stress, and just as important, provide them with peace of mind.
At the same time, “most people” benefit from the same level of care, even if they are not, or not aware of being, chemically sensitive.
Bad actors
There are a few common dental materials that are totally out of the pale, that should never be used. Mercury amalgam – ‘nuff said, but don’t forget the importance of careful barrier techniques when removing them, to protect patient, doctor and staff from mercury exposure during the procedure.
Nickel allergy is so prevalent in the population that its use in dentistry is outrageous. Unfortunately, due to a difference in immune response between skin and mucosa, the same nickel alloy that would make one’s skin break out if used in an earring, will not cause a rash in the mouth. So it’s hard to point to an obvious problem with the stuff. But it does raise the total level of immune reactivity in the body, and should not be used.
This calls into question the safety of stainless steel crowns, especially the NiCro variety. Also, nickel and other non-precious metal alloys tend to contribute disproportionately to galvanic electricity in the mouth.
Immune reactivity
Dental materials implanted in teeth present a systemic exposure, which implies the possibility of an immune response. Two clinical labs provide “serum compatibility testing” for dental materials, which involves testing blood serum for pre-existing antibodies to the more than 140 metals and chemicals that can be found in dental materials. Each chemical is graded according to whether it creates clumps in the serum or not. If it clumps, there’s an antibody against it. If there’s no clump, there’s no antibody reacting.
A computer program then reassembles those components into thousands of name-brand products. If there is a reactive chemical in the product, it is flagged and labeled not acceptable. Both labs provide a booklet of results by product name and by category.
The two labs are:
Clifford Consulting Laboratory, www.ccrlab.com, 719-550-0008
Biocomp Laboratories, www.biocomplabs.com, 800-331-2303
There are a couple of differences between the two labs. Biocomp grades products in three levels, “highly reactive,” “moderately reactive,” and “least reactive.” Clifford grades products in a binary fashion as either “satisfactory” or “unsatisfactory.”
An important difference lies in the two labs’ interpretation of aluminum sensitivity. Aluminum is very common in dental materials, and Biocomp treats all aluminum the same, as a problem. Therefore they kick out most porcelains and ceramics when aluminum sensitivity is detected. Clifford, on the other hand, regards insoluble aluminum compounds such as aluminum oxide and aluminum silicate as not biologically available, so products that contain aluminum in those forms are not graded “unsatisfactory” even if aluminum antibodies are detected. Therefore, many more ceramic brands end up on the good list in Clifford reports.
Both labs have very informative websites, and both are very willing to discuss their techniques and preferences. The owners of both labs are longtime IAOMT members, too.
Serum compatibility routines
After deciding which lab you want to use, obtain test kits, or have them sent directly to the individual patient. Provide the patient with a prescription for blood draw, unless you do that yourself. The patient takes the kit to a nearby blood lab, such as Quest Diagnostics, Labcor, or a local hospital. The patient fills out the enclosed paperwork and includes a check. The blood lab draws one tube of blood, prepares frozen serum, and overnights the sample to the compatibility lab. It’s best to draw the sample early in the week, so Biocomp or Clifford can receive it before the weekend. Both labs are quick at getting the results back to you.
Clifford Consulting Lab will also maintain a list of your favorite materials, and the results for those will appear on the front page of the report.
Who should get tested? Some of our members test all new patients, while others test only those who have documented MCS problems. That’s a clinical judgement call.
Multiple lenses
The sicker or more sensitive the patient, the more reassurance they need about the safety of our materials. Frankly, the differences among most current composites are minimal, and it probably doesn’t matter which you use for healthy patients. For the true MCS patient, or the suspected, or the nervous, there are more lenses that can be brought to bear on the compatibility question.
If you have a list of acceptable materials from a Biocomp or Clifford test that fits into your range of clinical choices, you might give the patient a physical sample of the proposed filling or crown, etc., to take home and try for themselves, in a fully reversible fashion. Remind them that this material has passed the blood test, and tell them to hold it in the cheek for a few minutes, or a few hours, and see if a familiar reaction starts. Taping a sample to the skin can be a revealing test, but it must be accompanied by a blank control.
Some people subscribe to the more “holistic” methods, like muscle testing or electrodermal testing. The patient can take your physical sample to another practitioner, too, for this type of corroboration. (It helps if you know the other practitioner, because once in a while, dealing with someone who does not understand dentistry can lead to more confusion, rather than more clarity.)
To whatever extent there is a psychological component to chemical sensitivity, going through all these motions for compatibility testing will go a long way toward reassuring that sensitive patient, and recruiting his or her belief system.
In the end, you as a licensed dentist, must decide your own comfort level, and adjust your techniques accordingly.
Problems with metals
Metals are much more allergenic than we typically give them credit for. Does anyone remember being told in dental school to ask patients, especially women, if their skin breaks out with jewelry? Very few patients ever report having been asked that by a dentist.
It is more possible than ever to perform good dentistry without the use of any metals at all, but sometimes we still need them. Some metals, most notoriously nickel, will create contact dermatitis, or a skin rash, upon exposure, and these are easily discovered by history and by serum testing. Other metals, most notoriously titanium, will never make a skin rash, but can lead to other manifestations of type IV delayed hypersensitivity, a much more insidious cause of malaise and other vague varied symptoms.
For patients where you plan a metal-based prosthodontic procedure, especially if there is any history of metal sensitivity, the most revealing test is the Melisa test (www.melisa.org). This is the only test that will show titanium sensitivity. (Of those tested, only 4% have tested positive to titanium on Melisa.)
Melisa is short for “memory lymphocyte activation,” and it takes four to six tubes of blood to get enough cells. The cells are isolated and cultured with the suspected antigen and tritiated thymidine. Cell proliferation, uptake of radioactivity, and morphological changes are taken as evidence of reaction. The Melisa test was created by immunologist Vera Stejskal, PhD, of Sweden, who has been a frequent speaker at IAOMT meetings.
Several labs around the world perform this test, and are listed on their website. One lab in North America performs Melisa:
Pharmasan Laboratory, www.pharmasan.com, 715-294-1705
Avoiding oral galvanism
Aside from their power to provoke immune reactivity, metals are also electrically active. Oral galvanism has been talked about for well over 100 years, but dentists generally ignore it and its implications.
Remember the electromotive scale from inorganic chemistry? Remember the potato clock, where a copper nail and a zinc nail stuck in a potato make enough electricity to run a digital clock?
Here are some representative voltage numbers (standard hydrogen electrode) for typical dental metals:
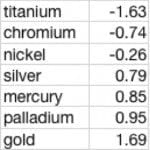
This means that gold and titanium grouped together in an electrolyte like saliva have the potential to create a battery of over three volts! (This is very oversimplified, go ask a corrosion chemist!) But considering that the nervous system works on membrane potentials of 0.140 volts, electricity from dental metals that is conducted randomly or unpredictably through anatomical structures and spaces can overwhelm normal neuronal control. Often the manifestation is localized pain, or inappropriately elevated muscle tone, – as in jaw tension, TMJ, temporal headache, skin pallor due to low level vasoconstriction, etc.

Why do the best stories still come from the old student days? I was covering the ER oral surgery clinic one Sunday afternoon when a homeless, disoriented woman came in. Her complaint was that the aliens in flying saucers were sending poison rays into her face, and they were spreading down her arm. I figured there must be some reason she was in my clinic, so I looked in her mouth. She had the typical assortment of metal restorations, some non-precious crowns, some gold crowns, amalgam fillings, all topped by a cast metal partial denture. You could almost see sparks when she bit down. “Poison rays from space!” I had her remove the partial, and bite. “No poison rays!” Put the partial back in. “Poison rays from space!”
Avoid poison rays from space. Don’t be cavalier about mixing metals in people’s mouths. The old standard in the gold days would have been to make all restorations in a person’s mouth, including removable frameworks, from the same high noble alloy, and not to mix metals at all. Now we can choose flexible nylon-base partial dentures, all-ceramic crowns and bridges, even ceramic implants – all the contemporary non-metallic methods we are currently blessed with, and all the ways we can do our jobs while walking more softly through our patients’ lives.
Steve Koral, DMD, MIAOMT
___
https://iaomt.org/practical-guide-compatibility-testing-dental-materials/