
PAIN, INFLAMMATION, ADENOSINE AND PEMF THERAPY
DrPawluk.com
A critical consideration for selecting and applying pulsed electromagnetic field (PEMF) therapy is the strength of the magnetic field needed to affect the tissue being treated. For the most effective results, the individual seeking to do PEMF therapy needs to determine three factors:
- The goal magnetic field intensity
- The length of treatment
- The number of sessions needed for the target tissue to be treated
PEMF Therapy is a developing medical field and there are no clear cut guidelines available for the myriad of conditions and circumstances for which people can and are likely to want to use PEMF therapy. One thing is clear though, one “size” does not fit all.
Another critical consideration is the intensity of the magnetic field at a distance from the applicator. For this calculation, apply the inverse square law. This law dictates that the magnetic field, normally, rapidly reduces in intensity with distance from the source of the field, that is, by the inverse square root. (Also see Intensity Matters Video)
TREATING CHRONIC INFLAMMATION WITH PEMF THERAPY
One of the most common uses of PEMFs is to reduce chronic inflammation. Inflammation is at the root or a major part of a majority of health conditions in humans and animals. This blog provides an example of the magnetic field intensities required to adequately treat inflammation throughout the body. Because of their actions on inflammation, PEMFs have been found to help with a number of other health conditions as well: infection, pain, sleep problems, arthritis, bone stimulation (fractures and bone surgery), cancer, ischemia, wound healing, and problems with the eyes, liver, lungs, heart, and nervous system, among many other tissues.
ADENOSINE: THE INFLAMMATION “GUARDIAN ANGEL”
A very important part of control of inflammation is through a molecule in the body called adenosine acting through its receptor, the adenosine receptor (AR). Adenosine is a building block for RNA/DNA and a part of the energy molecule ATP (Chen). Adenosine regulates the function of every tissue and organ in the body and is considered a “guardian angel” in human disease (Borea).
All cells release ATP at low levels. Release is enhanced with PEMF stimulation, inflammation, pH change, hypoxia, tissue damage, or nerve injury in all the tissues of the body. The mitochondria need adenosine to make ATP in all the cells of the body. Through various metabolic processes, adenosine is released by the breakdown of ATP to create energy and then is re-used to create more ATP in a perpetual cellular cycle.
HOW ADENOSINE, INFLAMMATION AND PAIN ARE LINKED
The concentrations of adenosine are naturally at physiologically low levels in body fluids between the cells of unstressed tissues. These concentrations increase rapidly in response to cell injury-causing stress conditions such as low oxygen (hypoxia), lack of blood supply (ischemia), inflammation, or trauma. Adenosine has a short half-life in the blood (a few seconds) and in spinal cerebrospinal fluid (10 to 20 minutes) (Antonioli). Adenosine is released from within the cell after production of ATP by mitochondria inside the cell (intracellular space) and then passes through the cell wall into the spaces between cells (extracellular space). Once released into the extracellular space, adenosine functions as an alarm or danger signal; hence a “guardian angel.” It then activates specific adenosine receptors, causing numerous cellular responses that aim to restore tissue homeostasis.
Adenosine acts through four subtypes of adenosine receptors: A1, A2A, A2B and A3.
These receptors are widely distributed throughout the body and have been found to be part of both physiological and pathological biological functions. They affect, at the least, cardiac rhythm and circulation, breakdown of fat, kidney blood flow, immune function, regulation of sleep, development of new blood vessels, inflammatory diseases/inflammation, blood flow, and neurodegenerative disorders. ARs are found in many types of immune cells, including neutrophils, macrophages, dendritic cells, and mast cells.
PEMF THERAPY FOR INFLAMMATION AND PAIN
PEMFs appear to primarily influence A2A and A3 ARs. They do not appear to influence A1 or A2B ARs (Varani, 2002). PEMFs stimulate the activation of adenosine receptors, increase their functionality, and augment chemical agents that also stimulate these receptors.
Stimulation of A2A and A3 ARs by PEMFs in cells throughout the body results in reduction of inflammation by lowering many proinflammatory tissue cytokines, including reduction of:
- The levels of tumor necrosis factor-α (TNF-α)
- Interleukin (IL): IL-1β, IL-6, and IL-8 in microglial cells (Vincenzi, 2017)
- IL-6 and IL-8 in cartilage and bone cells (Vincenzi, 2013)
- IL-8 and NF-kappa B in skin cells (Vianale)
- Synovial fibroblasts (Ongaro)
But very low intensity PEMFs between 3 and 5 microTesla (μT) do not affect IL-1β, IL-6, TNF-α, IL-8, or IL-10 production (de Kleijn).
Most research todate has been done on PEMF stimulation of A2A ARs. PEMF stimulation of A3 ARs specifically could benefit bone marrow and lymphatic disorders and gastrointestinal and various skin conditions.
THE ANTI-INFLAMMATORY EFFECT OF PEMF THERAPY
PEMFs stimulate the production of adenosine by stimulating A2A receptors, being especially helpful in chronic inflammation (Palmer). A2A receptor stimulation and adenosine produce most of their immune benefits through the T cell immune system. A2A receptors’ inhibitory effects on immune and inflammatory processes are very complex. Basically, the A2A receptor is, normally, naturally stimulated by acute inflammation-producing molecules to inhibit or control the inflammation. When adenosine production drops off or is low, inflammation persists and produces chronic inflammation.
In fact, PEMFs, by increasing ARs, enhance the functional efficiency of adenosine, resulting in a stronger physiological action than the use of drugs. The anti-inflammatory effect of adenosine enhanced by PEMF is less likely to have the side effects, desensitization, and receptor resistance than drugs used to act on adenosine receptors. Prolonged stimulation of adenosine receptors with a drug can dampen the ability of the receptor to function. Prolonged use of drugs decreases the quantity of receptors, thereby reducing the effectiveness of the drug over time.
The role of adenosine receptors and adenosine in modifying inflammation is well accepted (Varani, 2017). A2A receptors are plentiful in the membranes of neutrophils. Neutrophils play a major role in inflammation and tissue repair. Neutrophils are about 40% to 70% of white blood cells in most mammals. They form an essential part of the innate immune system. The innate immune system is one of the two main immunity strategies; the other is the acquired or adaptive immune system. Like the innate system, the acquired system includes both circulating and cell-based immunity. Neutrophils are recruited to a site of injury within minutes following trauma and are the hallmark of acute inflammation. Neutrophils are one of the first responders of inflammatory cells to migrate toward the site of inflammation.
THE BEST PEMF THERAPY FOR PAIN AND INFLAMMATION

Stimulating the A2A adenosine receptor on the neutrophil is essential for controlling inflammation. Because PEMFs stimulate the A2A receptor, determining the appropriate dose of the magnetic field is critical for optimal benefits. PEMFs applied in the lab at the surface of neutrophils have been found to significantly increase the binding of adenosine to the A2A receptor. This effect was time, intensity, and temperature dependent. PEMF dose-response studies have found that after 30 minutes of exposure, the receptors became saturated with a 1.5 mT magnetic field (Massari). The effect plateaued with intensities greater than 1.5 mT (Figure 1). This means that intensities above 1.5 mT produce no additional benefit, although they do not appear to have any negative actions either.
Figure 1. Saturation binding of A2A adenosine receptor as a function of magnetic field peak intensity (mT) in human neutrophil membranes. Bmax = receptor binding capacity. Adapted from Massari (2007).
The PEMFs used in this research had an intensity range from 0.1 to 4.5 mT; frequencies ranged from 10 Hz to 120 Hz. The most used peak intensity of the magnetic field was 1.5 mT (15 Gauss) at 75 Hz.
Armed with this information, 1.5 mT would be the optimized intensity of a magnetic field needed to help with reducing inflammation, at least as far as neutrophil involvement is concerned. When considering that individuals applying PEMFs for various problems associated with inflammation, the need is to be able to reduce inflammation at various depths in the body, depending on the target organ and tissue. Therefore, the intensity of the magnetic field of the applicator always needs to be considered in the decision making.
To achieve the 1.5 mT goal, PEMF intensity acting on neutrophils at various distances from the applicator—that is, at various depths into the body—the clinician must be aware of the inverse square law governing the loss of magnetic field intensity with distance from the applicator.
Table 1 was calculated for the 1.5 mT goal intensity at various depths in the body, using Newton’s inverse square rule.
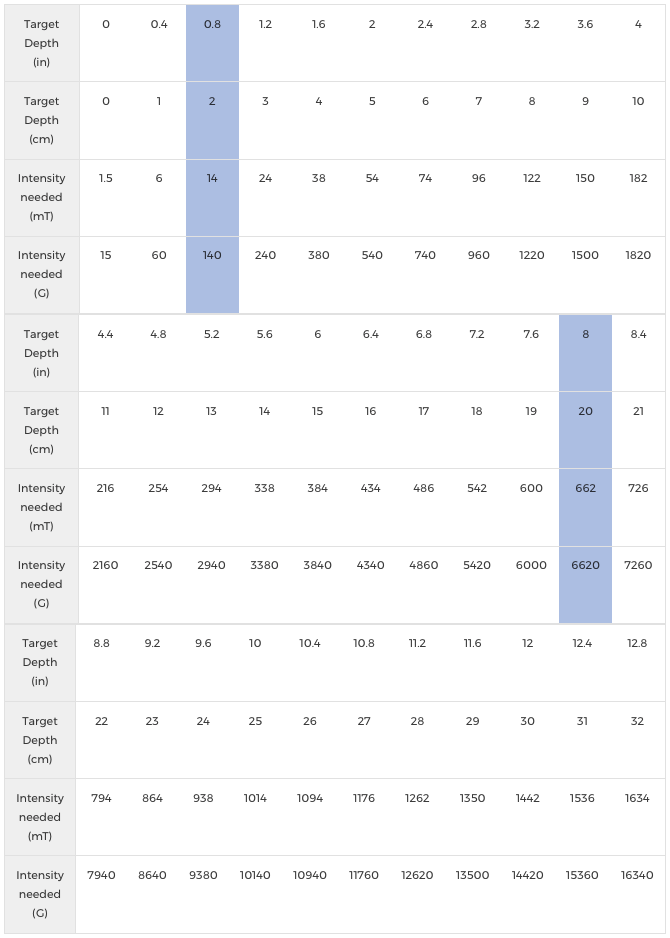
From the table, it can be seen, for example (in the blue areas), that to deliver 1.5 mT (15 Gauss) to the target tissue 2 cm (0.8 in) from the applicator, a 14 mT (140 Gauss) intensity magnetic field would be required. At 20 cm (8 in), 662 mT (6620 Gauss) would be required to deliver 1.5 mT (15 Gauss) at the target tissue.
TARGETED PEMF THERAPY FOR SPECIFIC CONDITIONS
To give an example, the kidneys may be a target for PEMF treatment. Inflammation in the kidneys is common, and the kidneys have been found to have adenosine receptors. We know that neutrophils are present within the kidney circulation when there is inflammation. The depth of the center of the kidneys into the body is typically from 5 to 7 cm (2 to 2.8 in) from the front of the abdomen (Xue). The thickness of the kidneys is typically about 5 cm (2 in) from the center of the kidney to the back of the kidney (Moorthy). If a PEMF applicator is placed over the anterior abdomen and the expected depth to reach the back of the kidney is 9.5 cm—or rounding up, 10 cm (3.9 in)—with the goal intensity being 1.5 mT, the maximum PEMF intensity would need to be 182 mT (1820 Gauss). This means that a PEMF system would need to be selected that can deliver at least this much magnetic field intensity to adequately target the kidneys.
Similar calculations can be done for any organ or tissue in the body to determine the optimal PEMF intensity needed. All one needs to figure out is the depth of the tissue, not only at the surface of the organ but also across the diameter of the organ or tissue farthest from the PEMF signal. In treating the brain, for example, the skull may be 15.2 cm (6 in) front to back and 12.7 cm (5 in) side to side. That means to treat the brain from front to back would require a magnetic field intensity of around 384 mT/3840 Gauss, to deliver 1.5 mT/15 Gauss to the back of the brain. Side-to-side treatment would require about 294 mT/2940 Gauss.
Targeting the anti-inflammatory effects of adenosine receptor stimulation is only one possible consideration for selection of magnetic field intensity in judging magnetic field intensity needs. Because there are so many different physiologic effects and actions of PEMFs (see Power Tools for Health book https://www.drpawluk.com/product/power-tools-health/), dosing calculations for each of these effects are not available for the PEMF user. In addition, it is unlikely that any specific physiologic action – for example, enhanced circulation, accelerated healing, pain reduction – can be uniquely and specifically selected in considering actual applications in the clinical environment. Experience suggests that multiple actions are at play any time a PEMF is used.
AFFECTS OF PEMF THERAPY ON THE BODY THROUGH INDIRECT ACTION
A recent study (Cañedo) showed that diabetic foot ulcers could be helped by treating parts of the body other than the foot ulcers directly. ( https://www.drpawluk.com/pemf-studies/pemfs-for-healing-diabetic-foot-ulcers/) This indirect action can take longer (up to 60 days) to produce results than direct PEMF stimulation at the ulcer site. This means that stimulating neutrophils in one part of the body may activate the adenosine receptors circulating under the magnetic field sufficiently to benefit inflammation in other parts of the body. Direct stimulation of the ulcer would activate other mechanisms of healing action of PEMFs to result in faster healing, such as increased collagen production.
Nevertheless, even local treatment with a PEMF at sufficient intensities may help inflammation in the rest of the body indirectly. However, the adenosine stimulated by PEMFs has a very short half-life and would require frequent repeat treatments or treatments over extended periods.
SUMMARY
Using PEMFs to reduce inflammation in the body, which is common to a vast majority of health conditions, is assisted by a “guardian angel,” adenosine and the adenosine receptor. This new research, that shows an impact of PEMFs on this receptor, gives important guidance in choosing the magnetic field intensity necessary, in any areas of the body with inflammation, to produce the best results. We no longer have to resort to guessing about which magnetic field intensity to choose to best help the body to heal.
References
- Antonioli L, Blandizzi C, Pacher P, Haskó G. Immunity, inflammation and cancer: a leading role for adenosine. Nature Reviews Cancer 2013 (13): 842–857.
- Borea PA, Gessi S, Merighi S, Varani K. Adenosine as a multi-signalling guardian angel in human diseases: when, where and how does it exert its protective effects? Trends Pharmacol Sci. 2016 Jun;37(6):419-434.
- Cañedo-Dorantes L, Soenksen LR, García-Sánchez C, et al. Efficacy and safety evaluation of systemic extremely low frequency magnetic fields used in the healing of diabetic foot ulcers—phase II data. Arch Med Res. 2015 Aug;46(6):470-8.
- Chen JF, Eltzschig HK, Fredholm BB. Adenosine receptors as drug targets — what are the challenges? Nat Rev Drug Discov. 2013 April; 12(4): 265–286.
- de Kleijn S, Bouwens M, Verburg-van Kemenade BM, et al. Extremely low frequency electromagnetic field exposure does not modulate toll-like receptor signaling in human peripheral blood mononuclear cells. Cytokine. 2011 Apr;54(1):43-50.
- Massari L, Benazzo F, De Mattei M, et al. CRES Study Group. Effects of electrical physical stimuli on articular cartilage. J Bone Joint Surg Am. 2007 Oct;89 Suppl 3:152-61.
- Moorthy HK and Venugopal P. Measurement of renal dimensions in vivo: A critical appraisal. Indian J Urol. 2011 Apr-Jun; 27(2): 169–175.
- Ongaro A, Varani K, Masieri FF, et al. Electromagnetic fields (EMFs) and adenosine receptors modulate prostaglandin E(2) and cytokine release in human osteoarthritic synovial fibroblasts. J Cell Physiol. 2012 Jun;227(6):2461-9.
- Palmer TM and Trevethick MA. Suppression of inflammatory and immune responses by the A2A adenosine receptor: an introduction. British Journal of Pharmacology (2008) 153 S27–S34.
- Varani K, Gessi S, Merighi S, et al. Effect of low frequency electromagnetic fields on A2A adenosine receptors in human neutrophils. Br J Pharmacol. 2002 May;136(1):57-66.
- Varani K, Vincenzi F, Ravani A, et al. Adenosine receptors as a biological pathway for the anti-inflammatory and beneficial effects of low frequency low energy pulsed electromagnetic fields. Mediators Inflamm (2017) 2017:2740963.
- Varani K, Vincenzi F, Targa M, et al. Effect of pulsed electromagnetic field exposure on adenosine receptors in rat brain. Bioelectromagnetics. 2012 May;33(4):279-87.
- Vianale G, Reale M, Amerio P, et al. Extremely low frequency electromagnetic field enhances human keratinocyte cell growth and decreases proinflammatory chemokine production. Br J Dermatol. 2008 Jun;158(6):1189-96.
- Vincenzi F, Padovan M, Targa M, et al. A(2A) adenosine receptors are differentially modulated by pharmacological treatments in rheumatoid arthritis patients and their stimulation ameliorates adjuvant-induced arthritis in rats. PLoS One (2011) 8(1):e54195.
- Vincenzi F, Ravani A, Pasquini S, et al. Pulsed electromagnetic field exposure reduces hypoxia and inflammation damage in neuron-like and microglial cells. J Cell Physiol (2017) 232(5):1200–8.
- Vincenzi F, Targa M, Corciulo C, et al. Pulsed electromagnetic fields increased the anti-inflammatory effect of A₂A and A₃ adenosine receptors in human T/C-28a2 chondrocytes and hFOB 1.19 osteoblasts. PLoS One. 2013 May 31;8(5):e65561.